EHC Insights
In today’s healthcare environment, anesthesia subsidies are common hospital operational costs, often costing millions of dollars. With eighty percent of hospitals paying an anesthesia subsidy, finding ways to reduce these costs – without risking quality – is a hot topic. What’s more, anesthesia groups face decreasing reimbursements and, supply-demand imbalances that dramatically drive up subsidy requirements.
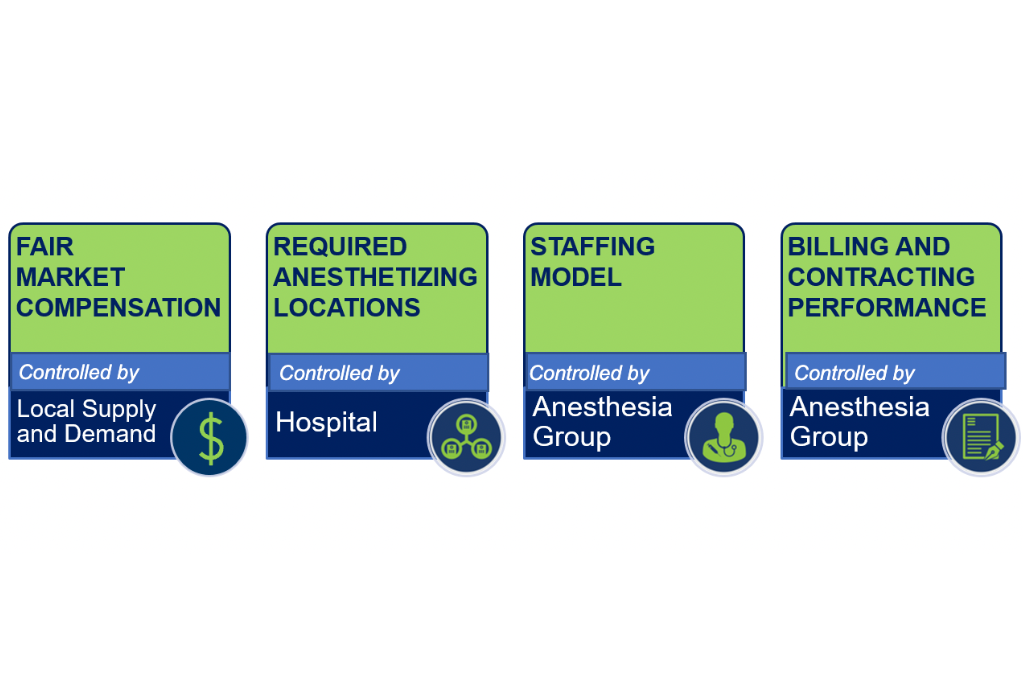
Contract negotiations should maximize the value of the significant investments hospitals make in their anesthesia service while supporting fair compensation for anesthesia providers. These discussions offer a chance to isolate and address any of the incongruities between anesthesia group needs and hospital budgets. However, to do so, facility leaders must understand the four drivers of anesthesia subsidies: Fair Market Value Compensation, Anesthetizing Locations, the Anesthesia Staffing Model, and Revenue Cycle Performance.
Fair Market Value Compensation
Fair market value compensation is based on several factors including geographic location, call requirements, case types and subspecialty training expectations. This value can be determined by comparing several regional surveys of salary and benefits packages, ranging from high to low, and not solely judging by the median rate. Supplemental modifications should be made after considering a number of factors such as the region’s average cost-of-living, case volume, call stress, and contract length. By identifying each of these factors a reasonable compensation allocation can be determined.
Anesthetizing Locations/ Providers
The number of anesthetizing locations directly plays into subsidy costs. Administrators are often pressured to open additional locations, or to provide numerous flip rooms for surgeons. However, in the absence of incremental cases to fully utilize the added capacity, with each location comes an increase in staffing costs, as well as a decrease in surgical minutes performed per location. This reduction means lower productivity and less billable hours per provider, which then expands the difference between provider expense and realized revenue. The additional subsidy necessitated by this capacity may be warranted, but that is ultimately a business decision driven by the ability to increase market share and incremental surgical cases.
Staffing Model
Whether an anesthesia group chooses a physician only, anesthesia care team, or CRNA only model, finding the right fit and balance in a staffing plan has a direct impact on subsidy. The chosen model can have a major impact on the subsidy requirements. However, choosing a staffing model is a complex decision requiring the consideration of a variety of factors: surgeon preferences, case complexity, call obligations, after hours workload and subspecialty coverage requirements. During negotiations, expert advice from individuals familiar with anesthesia staffing norms can be a valuable resource to help hospitals understand the staffing model complexities and opportunities.
Revenue Cycle Performance
While most contracted groups do their best to collect all amounts due to them from payers, anesthesia billing is unique and complex. Subsidizing based on a revenue guarantee without closely monitoring anesthesia billing is a common error. In this construct, ultimately hospitals assume the risk of poor revenue cycle realization. Ideally, facilities should monitor charge capture, payer contracting strategies, net collection percentages and receive monthly reports. In fact, even facilities with fixed anesthesia subsidies should ensure adequate anesthesia revenue cycle practices. Otherwise the group may come back with an unnecessarily high request for subsidy upon contract re-negotiation.
These four drivers can be evaluated and adjusted to identify opportunities for increasing collections and reducing costs – improving the hospital’s bottom line. EHC’s Anesthesia Subsidy Value Index takes key metrics from a hospital’s OR to determine if it is receiving the most efficient level of anesthesia coverage and highlights areas that can be improved upon.
To inquire about your anesthesia subsidy’s value, contact us today!
Written By: Howard Greenfield, M.D.
Subscribe to receive articles by email
Get notifed by email when we release new Insights!