Pre-Op Your Anesthesia Practice
More anesthesia groups than ever are about to undergo the business equivalent of an invasive procedure

Anesthesiologists routinely perform a “pre-operative” assessment of a patient scheduled to undergo an invasive procedure that requires anesthesia services. This assessment is a standard of care that has benefits that are guided by the provider’s intention to limit surprises. No physician wants to be in the middle of a complex surgical case and first find out about an underlying chronic condition that has deleterious effects on the patient. It is our observation that more anesthesia groups than ever are about to undergo the business equivalent of an invasive procedure. Shouldn’t you apply the same standard to your own practice, and find out how your group will look to a possible partner, investor or employer before your group is in the middle of negotiations with another entity? The radically changing healthcare world will confront all hospital-based anesthesia group practices with complex and difficult choices. Do you stay the course and try to postpone the inevitable, or pursue alternatives to the status quo? Either way, aren’t you better off mitigating the surprise factor now, rather than in the middle of a group take-over, merger, sale or offer of hospital employment?
There is no best single answer to any of the questions above. In fact, each option brings many additional questions to the forefront. One of the most important first steps is to perform a SWOT analysis (Strengths, Weakness, Opportunities, Threat) of your group. What are your group’s strengths and weakness? Do you have hospital contracts, and how secure are they? Are there opportunities, such as partnering with other similarlysituated groups? What are the real versus imagined threats? For example, is your hospital really interested in forcing employment on your group or is the hospital just tired of dealing with difficult members of your group? Where are your threats coming from, and do you have the ability to recognize them from the inside? Many small- to medium-sized groups are worried about the larger anesthesia group across town and fail to realize that the more likely threat comes from within their own hospital system. With hospital margins rapidly decreasing, hospital administrators are looking for different ways to minimize the physician spend at their facility.
In the past, a good anesthesia group providing quality services at the lowest possible cost would not have to worry that a competitor could underprice them without reducing services. That is no longer true, as more entrepreneurial physician organizations have a menu of hospital-based specialties to offer: Emergency, Radiology, Intensivists, etc. The opportunity for such a group is to use the substantial profitability of the other hospital-based services to “pay down” the anesthesia subsidy. This type of marketing has opened a whole new world of competitive bidding. These same large multi-specialty groups often have geographic leverage with payers and favorable national contracts to substantially increase anesthesia revenue and decrease the subsidy for their hospital customers.
In order to decide which route may be best for your group, let’s go back to the common starting place where all anesthesiologists begin patient care—the anesthesia pre-op assessment.
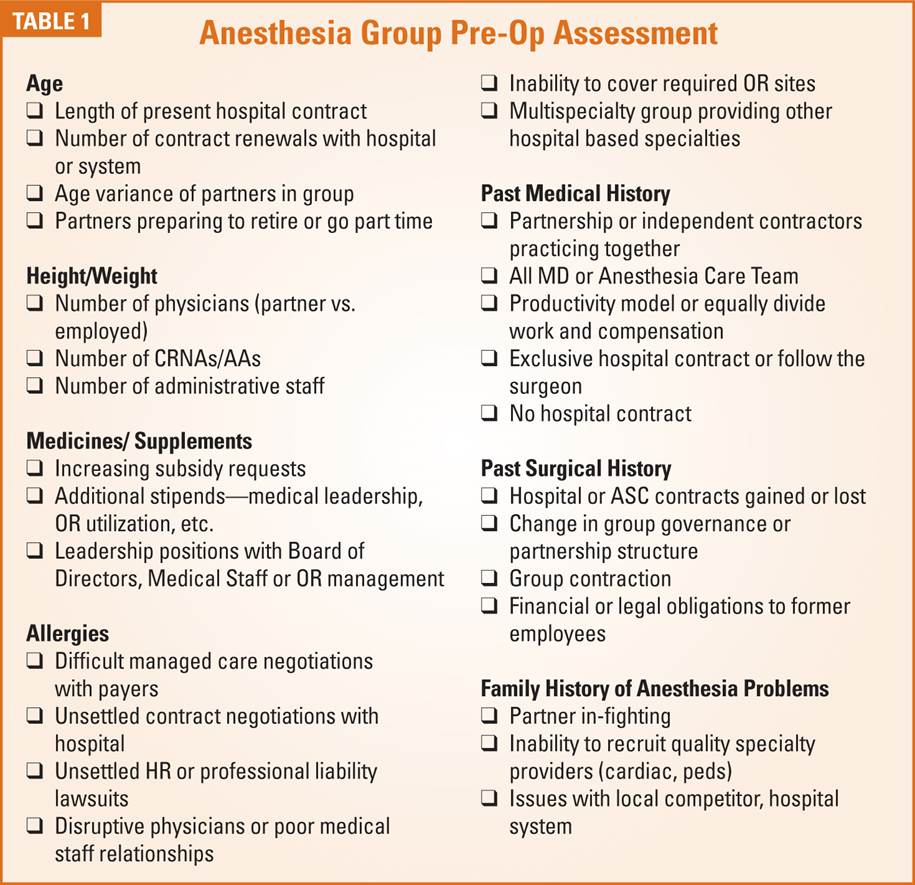
As you fill out your Anesthesia Pre-op Assessment sheet, remember to check the boxes that best describe your present anesthesia practice. (See Table 1 on page 4). Truthful answers to these questions will help you determine your anesthesia group’s ASA status—its Ability to Sell to Another. This is equally important in retaining your present contract or marketing your group to a hospital system, individual facility, national buyer or regional partner.
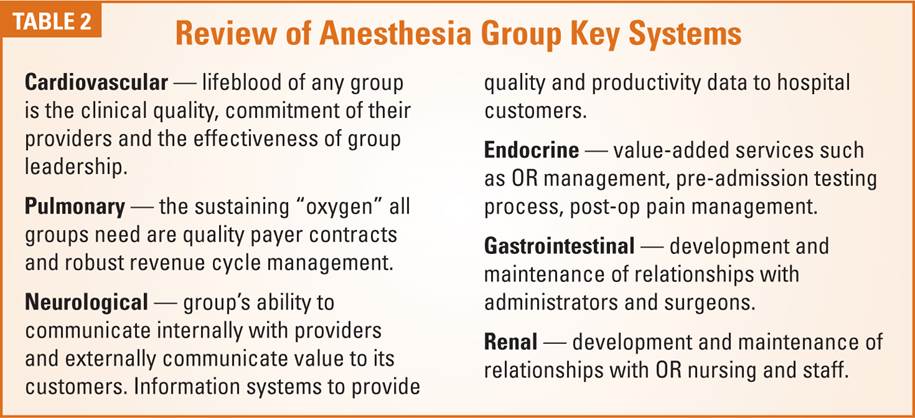
In the typical anesthesia pre-op process, the review of systems follows the collection of pertinent patient data and past medical and surgical history. As you begin to review your own group, it is important to look at and determine how well the key systems are functioning in your practice. (See Table 2). In many cases groups will need to bring in outside consultants to help them thoroughly evaluate a particular system.
At this point a simple question to pose to your group is, “If our practice sold shares to investors, with a promise of return on that investment, would you buy additional shares of our own practice?” Whatever the initial reply to that question, isn’t it incumbent on the partners or owners to determine “pre-operatively” what value the practice may have before potential investors or employers are about to “operate”?
Originally published here : anesthesiallc.com